I got the idea for this paper after analyzing what factors predicted vaccination rates in Kenya. I used 2014 DHS data (DHS is a nationally representative survey which is conducted in many countries that collects data on socioeconomic, health-related, and vital statistics). Regression analysis of non-vaccination against different sociodemographic variables showed that children of Somali ethnicity aged 12-23 months had 23-times higher odds of being non-vaccinated (receiving no vaccines at all) vs. being fully vaccinated. Full vaccination was defined as receiving all vaccines recommended by the Kenyan Ministry of Health’s Expanded Program on Immunization: 1 dose BCG (childhood TB vaccine), 3 doses oral polio, 3 doses pentavalent (a 5-antigen combo which contains Hepatitis B, Hib (Haemophilus influenzae type b, which can cause meningitis), and diphtheria, tetanus, and pertussis), and 1 dose measles.
Finding 23-fold odds is really noteworthy – and led me to investigate the drivers of this extreme disparity in vaccination rates among Somali children in Kenya.
Context is critical to pursue this research question – and that means understanding the political situation in East Africa.
The North Eastern region of Kenya is home to the Dadaab refugee camp, the largest refugee camp in the world. Established in 1991, it now houses almost half a million refugees. Civil unrest and conflict in Somalia have fed refugees into bordering countries, including Kenya, which houses more refugees (>300,000) than any neighboring country.
Refugees face more barriers to accessing healthcare than other residents. Refugees may lack familiarity with national customs, be harder to reach, be reluctant to use government services or encounter significant societal discrimination when trying to interface with the health system. All these factors adversely affect the likelihood of receiving proper and timely vaccinations.
The combination of this unique political context and the systemic barriers to health access that refugees face piqued my interest in further exploring the predictors of non-vaccination for Somalis in Kenya. In particular, whether the predictors would be different for Somalis than non-Somalis. If there were different predictors for this ethnic minority, this could point towards the existence of some of these systemic barriers and/or help to inform policy.
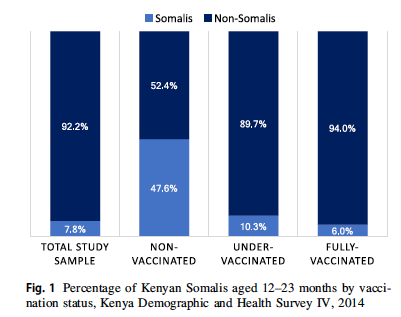
Ultimately, only 61.9% of Somalis were completely vaccinated, compared to 80.1% of non-Somalis. This disparity persisted for each individual vaccine, and all differences were significant (p < 0.001). Although only 7.8% of the full sample were Somali, Somalis represented 47.6% of those who were non-vaccinated – i.e. the children who received zero immunization services at all. This means that almost half of those aged 12-23 months in Kenya who are receiving zero vaccines are Somali, pointing to significant access disparities.
Our research team wondered whether common predictors of vaccination outcomes – wealth, gender, rural/urban environment, and birth setting – would affect Somalis and non-Somalis differently. To explore this, we performed an interaction analysis, examining how each of these variables interacted with Somali ethnicity to affect vaccination status. The results were surprising and presented some actionable policy implications. They also highlighted the importance of birth setting and maternal decisions on vaccination outcomes.
Wealth. In most studies, increasing wealth leads to better vaccination outcomes. We observed this trend among non-Somalis, but no such trend among Somalis. We believe this might indicate that Somalis in Kenya are facing significant cultural and access barriers to vaccination, which cut across all socioeconomic levels. This has implications for potential actions to address vaccination disparities. While programs designed to assist poorer segments of Kenyan society may improve vaccination outcomes among non-Somalis, they may be less effective for Somalis.
Birth setting was found to be a significant predictor of vaccination rates for both Somalis and non-Somalis. Those born in non-institutional settings, particularly with a traditional birth attendant or no birth attendant, have worse vaccination outcomes. We believe this might be because those born in non-institutional settings have reduced access to health professionals to vaccinate the child and/or convey vaccine information to the mother. In addition, babies born at home or in another non-institutional setting are not surrounded by other children receiving vaccines, as would happen in a hospital. This may make mothers less likely to vaccinate their children.
Since mothers’ decisions drive vaccination outcomes, and the recommended childhood vaccination schedule begins at birth, with BCG (the childhood TB vaccine), ensuring that mothers adhere to the vaccination schedule as early as possible improves the health of everyone. This is a problem given that 20% of the survey population, and nearly 60% of Somalis in the sample, had a non-institutional birth with a traditional birth attendant (TBA). Previous literature shows that many Kenyans rely on TBAs despite their lack of formal medical training. At first, we believed this presented an easy solution — train TBAs to deliver vaccinations, and voila! However, thanks to the input of our Kenyan collaborators on the paper, we learned that allowing TBAs to perform any medical tasks would be politically and culturally impossible. While the Kenyan government has tried to shift preferences towards skilled birth attendants and midwives, these have not been very popular. After discussions with our collaborators, we determined that training TBAs to provide vaccine information might improve outcomes without crossing cultural lines.
This experience highlighted the importance of cultural competence in doing research and drawing appropriate conclusions. I felt extremely lucky to be able to discuss ideas with those familiar with the Kenyan context and culture, and believe it’s necessary to conduct global research with local representation.
Altogether, this research found rampant disparities in vaccination rates between people of Somali and non-Somali ethnicity in Kenya. While we do not know if the sampled individuals are refugees in the Dadaab camp or just Kenyans of Somali ethnicity in the North Eastern region (the DHS does not reveal the locations of their sampling), these individuals’ health is at greater risk because of these disparities and their access to lifesaving vaccines needs to be improved.

Leave a comment