
In the U.S., there are no federal vaccination mandates. Rather, it is the states that determine vaccination requirements which are imposed on children entering school. Worldwide, mandatory vaccination is actually not a common practice: a recent study found that of 193 countries surveyed, only 105 (54%) had evidence of a national mandatory vaccination policy requiring at least one vaccine. Of those, only 59% enforce penalties on individuals who do not comply.
As we watch COVID-19 spiral out of control, claiming over 4,000 lives in one day in the U.S. alone, it’s important to highlight one of the great paradoxes of vaccination, and of public health more broadly: they are victims of their own success. When public health interventions are successful and vaccine-preventable diseases are controlled, there are fewer cases and outbreaks. The perceived risk of contracting the diseases diminishes, enabling fears about vaccine adverse reactions to outweigh fears of the disease itself, and fueling complacency about maintaining a robust public health infrastructure. Due to incompetent leadership and high rates of vaccine hesitancy, COVID-19 vaccination efforts are frustratingly slow in the U.S. Could the COVID-19 vaccine be mandated if uptake fails to meet herd immunity thresholds? To understand the possibilities, the history of mandatory vaccination in the U.S. is instructive.
Mandatory vaccines held constitutional in landmark 1905 Supreme Court case
The history of both compulsory vaccination and exemptions goes back to the late 1800s, when individual states began passing laws making vaccines compulsory for schoolchildren. A landmark 1905 case, Jacobson v. Massachusetts, was brought by Pastor Henning Jacobson on the grounds that he and one of his sons had endured adverse vaccine effects. He refused to vaccinate his other children after moving to Massachusetts, despite such vaccinations being mandatory for school entry. He was fined $5 and refused to pay this fine. His case went all the way to the Supreme Court, which determined that public health vaccination mandates were constitutional, confirming states have police power to protect public health and safety, even if doing so subordinates individual liberties to the common good.
The constitutional basis for mandatory vaccines was affirmed in the 1922 case Zucht v. King. A young Rosalyn Zucht was excluded from entering both public and private schools in San Antonio, Texas after refusing her smallpox vaccination. The Supreme Court ruled that schools could refuse to admit students who failed to meet vaccination requirements. The Court’s affirmation of the constitutionality of these two cases set the stage for compulsory vaccination laws moving forward.
With growing mandates came new exemptions and a regulatory patchwork
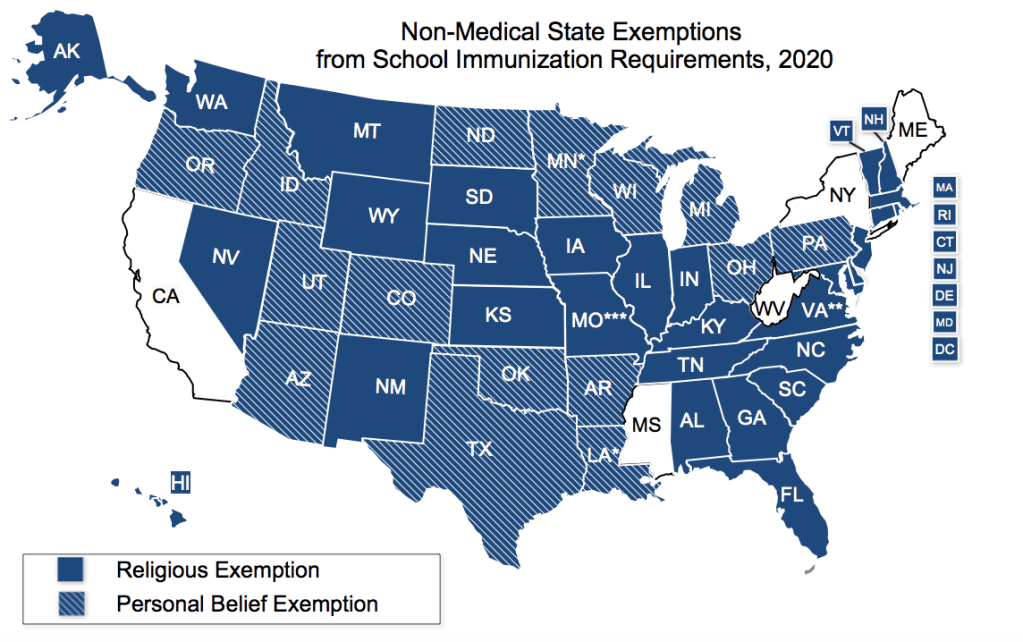
These landmark Supreme Court decisions affirmed the constitutionality of compulsory vaccination, but only a few states had mandatory vaccination requirements until the 1970s, when confronted with uncontrolled measles spread. By the early 1980s, all 50 states had some requirements making school entry for children conditional on immunization status. However, new state laws requiring mandatory vaccination led to the creation of new loopholes and exemptions. Differences in state exemption policies in turn produced a mixed landscape of vaccination exemptions across the U.S. All states allow for medical exemptions if a child had a true medical contraindication to vaccination, but some states also permit non-medical exemptions (NMEs) for religious and personal (philosophical) reasons, impacting parental decisions on where to live and send their children to school.
NME rates have been rising significantly across the U.S. in the past two decades. From 1991 to 2004, the average state-level NME rate in the U.S. increased from 0.99% to 2.54%. Philosophical exemptions have risen in 12 of the 18 states that allow them since 2009. However, exemption rates alone don’t tell the full story: where allowed, the ease of obtaining an NME also ranges from very restrictive to very permissive. At one extreme, Ohio parents can simply sign a note indicating their child has immunity or disease history, exempting them from vaccination. By contrast, Mississippi, which has not allowed NMEs since 1999, has had no reported cases of measles since 1992.
Rising NME rates have led to more stringent legislation to curb them
Legislation to address vaccination rules and exemptions has accompanied these rising NME rates, with 10 major legislative changes occurring from 2011-2016 across the US. Nine of these 10 policies made NMEs harder to obtain. Even more striking is how many pieces of legislation related to vaccine mandates and exemptions have been introduced in recent years, with 26 states introducing 70 bills from 2014-2018, though only 11 passed.
As of January 2021, all but 5 states (CA, ME, MS, NY, WV) offer NMEs for religious reasons, philosophical reasons, or both. Two of these states, New York and Maine, only just removed NMEs in 2019 after widespread measles outbreaks that year.
While reducing NME rates is important, another crucial way to protect community health is to reduce the spatial clustering of non-vaccinators, which can also drive outbreaks. In California, NME rates among kindergarteners increased from 0.73% in 2000 to 3.09% in 2013. This increase was accompanied by a concerning increase in geographic clustering, making outbreaks even more likely. In California, regions with high NME rates acted as seed locations, stimulating NMEs in nearby areas and showing evidence of social contagion. California responded with two separate pieces of legislation restricting the ease of exemptions. In 2014, California passed AB2109, which required parents to submit proof of discussing the risks of non-vaccination with a health care practitioner before obtaining an NME. AB2109 led to a small decrease in NMEs, but had no lasting impact on geographic clustering of exemptions, leaving communities in high exemption clusters at continued high risk of outbreaks.
A more stringent legislative effort in California went into effect just two years later: SB277 eliminated philosophical vaccine exemptions entirely, and following its implementation childhood vaccination coverage increased by 3% in the following year. However, as philosophical exemption rates plummeted, the rate of medical exemptions after SB277 increased by 300%, indicating that vaccine hesitant parents in California may have been acquiring medical exemptions from doctors willing to provide them.
Vaccine exemptions matter because they increase disease risk
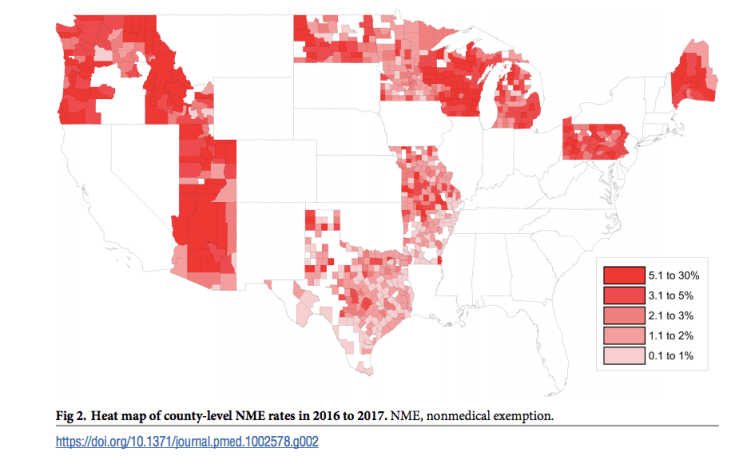
Spatial clusters of NMEs can predispose regions to outbreaks: Olive et al.’s 2018 study was surprisingly accurate at predicting hotspots for future measles outbreaks based on rates and geographic clustering of NMEs across the U.S. Therefore decreasing NME rates can protect communities from outbreaks, while increasing NME rates can endanger them.
Additionally, children with an NME are more likely to acquire and transmit vaccine-preventable diseases (VPDs): up to 35- and 6-times more likely to contract measles and pertussis, respectively. Thus NMEs increase the risk of both acquiring and transmitting infectious diseases, further solidifying the importance of pursuing more stringent NME regulation as an actionable public health measure.
The COVID vaccine is unlikely to be mandated in the U.S.
Vaccination is the best way to control disease – with vaccines responsible for the eradication of Smallpox, the near elimination of polio, and our best hope for ending the COVID-19 pandemic. However, growing anti-vaccine sentiment, vaccine hesitancy, and fears about infringement on personal and individual liberty make reaching herd immunity goals a daunting prospect. In light of this, could the COVID-19 vaccine be made mandatory for the general population?
It’s very unlikely – for a number of reasons. First, the vaccine was not even required for front-line health workers in phase 1A, the one group in which such a mandate would be fairly enforceable and which has precedents (the flu vaccine, for example). Second, such a mandate would be likely to cause huge blowback – as has been seen for state policies removing NMEs to pediatric vaccinations. Third, even mask mandates have caused significant backlash, with cries to preserve personal liberty above all else (including the public good). Finally, vaccination mandates have been deemed constitutional under Jacobson v. Massachusetts at the state-level only. States theoretically could mandate the vaccine for the general population, but are unlikely to do so: for all the reasons mentioned above and the difficulty of practically enforcing such a measure.
Instead – our national public health efforts should focus on improving vaccine uptake by combatting vaccine misinformation, bolstering confidence in vaccines, in science, and in public health, and improving the vaccine delivery infrastructure to get shots into arms faster. The more evidence we have that the vaccine is safe and reduces disease transmission, the more people will trust the vaccine.

Leave a comment