This paper explores the relationship between vaccine timeliness and co-administration using the Kenyan 2014 DHS. Why is vaccine timeliness important? Imagine we’re looking at vaccination coverage of 5 year-olds in Kenya, and we see that 92% of 5 year-olds received their measles vaccine. That looks great! However, imagine that in fact, only 70% of those 5 year-olds had received measles when they were supposed to, and the remaining 30% of those 5 year-olds got their vaccine at a catch-up nationwide measles campaign when they were 4. That means they had 3 years of unnecessary vulnerability to measles, and 3 years when they were at risk of getting sick and transmitting measles to others. This is why we think timely vaccination is a more important measure than merely vaccination coverage.
We used data from the DHS, or Demographic and Health Surveys, a massive statistical undertaking which implemented over 300 nationally-representative surveys in over 90 countries, asking questions about topics including fertility, family planning, maternal and child health (including vaccination), gender, HIV/AIDS, malaria, nutrition, and environmental health since 1984. Vaccine performance in a low-income country is often measured by coverage – simply how many people got all their recommended vaccines divided by how many people were eligible, yielding a simple proportion. However, timeliness is calculated by whether those vaccines were received according to their schedule, as determined by the Kenyan Ministry of Health (and often supported by the WHO). The vaccine schedule for Kenya can be seen in Table 1, below.
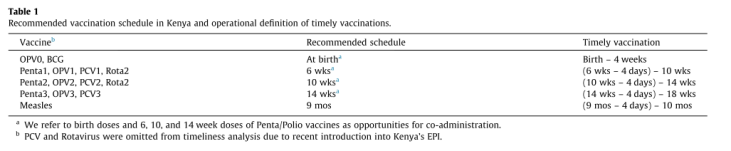
The Kenyan schedule requires OPV (oral polio vaccine) and BCG (Bacille Calmette-Guérin, the childhood TB vaccine) at birth. Then at 6 weeks, a second dose of OPV, along with doses of Pentavalent vaccine (includes diphtheria, tetanus, pertussis, Hemophilus Influenzae type B, and Hepatitis B vaccines), PCV (Pneumococcal conjugate vaccine), and Rotavirus Vaccine (prevents against childhood diarrhea). These same four vaccines are administered again at 10 weeks, and then again at 14 weeks though without rotavirus. The mothers are off the hook then until 9 months, when the children are due for their measles vaccination. In developing countries, many governmental programs use only measles-containing vaccine (MCV), not MMR, like we have in the US, and so are unprotected from Rubella and Mumps.
You can see from the schedule that the 6,10, and 14 week visits are biggies – kids are receiving four vaccines at their 6 and 10 week visits that protect them against 8 different important childhood preventable diseases. So a key component of receiving vaccines on time is receiving all the vaccines you’re supposed to at a given visit. If you receive 2 or 3 of the 4 recommended vaccines at 6 weeks, you’ll be late in catching up on the remaining vaccines, and research shows that often those children never fully catch up and complete the schedule like they’re supposed to. Reasons for not co-administering vaccines may be less the parent’s notion that ‘too many vaccines at once is a bad thing’, like we have in the US, and more related to supply side factors, like vaccine stock-outs, so this is a complex, but important issue.
There 10,385 children aged 1-4 years with vaccination cards included in the analysis. When we examined predictors of co-administration for the 6 week dose, we found that children in rural areas had nearly 1.5 x the odds of co-administration, and those who were in the poorest wealth quintile had 0.25 x lower odds of co-administration than those in the middle wealth quintile. Additionally, those born in non-institutional settings had consistently reduced odds of co-administration. What does this mean? If you live in a rural area, you may be more likely to visit only the public, government health center because that’s all that exists, which may make you more likely to get all your shots at once when you go with your child. Additionally, being very poor and having a home birth or traditional birth may set parents on a path for fewer interactions with the health system such that vaccines are not received appropriately.
But now the real question does co-administration improve timeliness? When we did an adjusted logistic regression to look at the odds of timely vaccination with each dose based on co-administration, we found that co-administering not only the dose in question, but earlier doses, increased the odds of timely vaccination! Gut check confirmed! This was the most noticeable for the birth dose, where those with co-administered birth doses had carry-over effects on timeliness throughout the schedule, all the way to the measles dose at 9 months!
It’s important to quickly discuss the limitations of this study – because we were examining timeliness, we needed the vaccination cards, which meant that those children without vaccine cards were not included. It is unlikely that this was a random difference, and so we cannot know how the selection bias would have affected our results. It is likely that those without vaccination cards were less timely, or did not receive their vaccines at all. Additionally, we did not have information on supply-side issues like vaccine stock-outs, which could have explained some of the reasons why vaccines were not co-administered.
Masters NB, Wagner AL, Carlson BF, Boulton ML. Vaccination timeliness and co-administration among Kenyan Children. Vaccine. 2018;36(11): 1353-1360. doi: 10.1016/j.vaccine.2018.02.001

Leave a comment